


posted 7th October 2025
In Part 1 of this series, we explored the science behind neurological physiotherapy, the principles of neuroplasticity, and the core components of effective rehabilitation programmes. We also reviewed the evidence showing why balance and strength training are vital in recovery.
In this second part, we take a closer look at condition-specific exercise approaches for stroke, multiple sclerosis, and Parkinson’s disease, before moving on to essential safety protocols, the role of technology in modern rehabilitation, and practical guidance for home programmes and multidisciplinary teamwork. If you’re looking to apply the evidence from Part 1 to real-world scenarios, this is where the pieces come together.
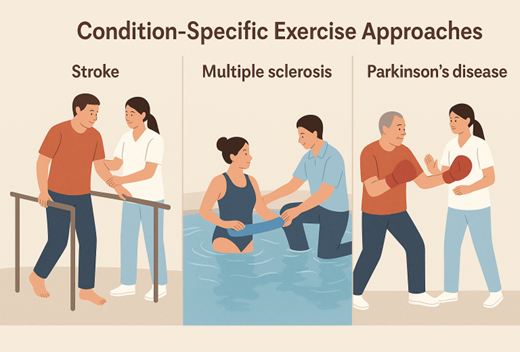
Condition-Specific Exercise Approaches
Stroke Rehabilitation Exercises
Stroke rehabilitation focuses primarily on addressing hemiplegia and motor recovery, with exercises designed to promote neuroplasticity and functional reintegration. Task-oriented training forms the foundation of stroke rehabilitation, involving practice of real-life activities such as reaching, grasping, and walking. Patients might practice pouring water from a pitcher or buttoning clothing, activities that integrate multiple motor and cognitive functions.
Constraint-induced movement therapy represents an evidence-based approach where the unaffected limb is restrained, forcing use of the affected side. This technique has shown remarkable success in improving arm and hand function, with studies demonstrating significant improvements in motor control and daily function use of the affected limb.
Gait training for stroke patients often begins with weight-bearing exercises and progresses to supported walking using parallel bars or harnesses. The focus is on reestablishing normal walking patterns, addressing issues like foot drop, hip hiking, and asymmetrical step length. Treadmill training with partial body weight support allows patients to practice walking movements safely while gradually increasing weight-bearing demands.
Multiple Sclerosis Exercise Programs
Multiple sclerosis exercise programmes must carefully balance activity with fatigue management, as MS patients often experience significant fatigue that can worsen with overexertion. Exercise sessions are typically scheduled during patients’ peak energy periods and include frequent rest breaks to prevent symptom exacerbation.
Aquatic physiotherapy proves particularly beneficial for MS patients, as the water’s buoyancy reduces gravitational stress while providing resistance for strengthening. Water temperature is carefully controlled to prevent overheating, which can temporarily worsen MS symptoms. Swimming and water walking exercises improve cardiovascular fitness while maintaining joint mobility.
Flexibility and stretching exercises address the muscle stiffness and spasticity common in MS. These might include gentle stretching of hip flexors, hamstrings, and calf muscles, performed slowly and held for extended periods. Heat application before stretching can enhance muscle relaxation and improve range of motion.
Parkinson’s Disease Interventions
Parkinson’s disease exercise programmes specifically target bradykinesia (slowness of movement) and freezing episodes that characterize this condition. Large amplitude movements are emphasized, as research shows that practicing big, exaggerated movements can help overcome the tendency toward small, shuffling steps and reduced arm swing.
Rhythmic exercises using external cues help patients overcome movement initiation difficulties. Marching to music, stepping over lines on the floor, and using metronome beats provide auditory and visual cues that can break through freezing episodes. These cueing strategies are particularly effective for improving gait initiation and maintaining walking rhythm.
Boxing-inspired exercises have gained popularity in Parkinson’s treatment, combining cardiovascular conditioning with complex motor movements. These programmes incorporate punching movements, footwork patterns, and balance challenges that address multiple symptoms simultaneously while providing an engaging, motivating activity.
Voice and breathing exercises complement movement training, as Parkinson’s often affects speech volume and respiratory function. Loud voice exercises combined with large arm movements can improve both communication and motor function through shared neural pathways.
Safety Protocols and Assessment Guidelines
Safety considerations are paramount in neurological physiotherapy, given the complex medical histories and functional limitations of patients with neurological conditions. Comprehensive pre-exercise screening procedures ensure that patients can safely participate in exercise programmes while minimizing risk of adverse events.
Medical clearance requirements vary depending on the specific neurological condition and associated comorbidities. Patients with recent stroke require cardiac clearance due to increased cardiovascular risk, while those with multiple sclerosis need assessment of heat sensitivity and fatigue patterns. Spinal cord injury patients require evaluation of autonomic function and skin integrity to prevent complications during exercise.
Fall risk assessment forms a critical component of initial evaluation, using standardized tools like the Berg Balance Scale and Timed Up and Go test. Environmental safety modifications include clear pathways, appropriate lighting, and readily accessible support surfaces. Exercise areas should be equipped with emergency call systems and have clear protocols for responding to medical emergencies.
Vital sign monitoring during exercise sessions helps identify signs of overexertion or medical complications. Blood pressure, heart rate, and oxygen saturation should be monitored before, during, and after exercise sessions, particularly in patients with cardiovascular comorbidities or autonomic dysfunction. Specific parameters for stopping exercise include excessive heart rate elevation, significant blood pressure changes, or patient reports of chest pain or severe shortness of breath.
Contraindications for neurological exercise include unstable medical conditions, severe cognitive impairment that prevents safe participation, and acute infections or illnesses. Relative contraindications require careful consideration and modified approaches, such as severe spasticity that might benefit from pre-exercise stretching or medication timing adjustments.
Emergency procedures should be clearly established and regularly practiced by all staff members. These protocols include recognition of medical emergencies specific to neurological conditions, such as autonomic dysreflexia in spinal cord injury patients or seizures in traumatic brain injury patients. Staff should be trained in basic life support and have immediate access to emergency medical services.
Regular reassessment ensures that exercise programmes remain appropriate as patients’ conditions change. This includes monitoring for disease progression in degenerative conditions like multiple sclerosis or Parkinson’s disease, as well as recognizing improvements that allow for exercise progression. Physiotherapists should maintain detailed records of patient responses to exercise and any adverse events to inform ongoing treatment decisions.
Technology Integration in Neurological Physiotherapy
Technology integration has revolutionized neurological physiotherapy, offering innovative tools that enhance traditional exercise approaches and provide new opportunities for motor learning and functional recovery. These technological advances enable more precise measurement, increased motivation, and expanded access to rehabilitation services.
Virtual reality applications have emerged as powerful tools for balance and gait training, creating immersive environments that challenge patients while maintaining safety. VR systems can simulate real-world scenarios like crossing streets or navigating crowds, allowing patients to practice functional skills in controlled settings. Research shows that VR-enhanced balance training can improve adherence to exercise programmes by 15-20% compared to traditional approaches.
Robotic-assisted devices support movement rehabilitation by providing precise, repeatable movements that help retrain motor patterns. Devices like robotic gait trainers allow patients with severe mobility limitations to practice walking movements with full support, gradually reducing assistance as function improves. Upper extremity robots help stroke patients practice arm and hand movements with precise force feedback and movement guidance.
Biofeedback systems enhance motor learning by providing real-time information about movement quality and performance. Surface electromyography (EMG) can show patients muscle activation patterns, helping them learn to activate weak muscles or reduce unwanted muscle tension. Balance feedback systems provide visual or auditory cues about weight distribution and postural sway, facilitating more effective balance training.
Mobile applications and home-based exercise monitoring extend rehabilitation beyond clinic sessions, allowing patients to continue structured programmes at their own pace. These apps can provide exercise reminders, track progress, and even use smartphone sensors to monitor movement quality during home exercises. Some applications include video conferencing capabilities for remote physiotherapist guidance and support.
Functional electrical stimulation (FES) combined with exercise creates hybrid interventions that can activate paralyzed muscles while patients attempt voluntary movements. This approach is particularly beneficial for spinal cord injury patients, allowing them to exercise muscles that would otherwise be inaccessible. FES cycling systems enable cardiovascular and strength training even in patients with complete paralysis.
Wearable sensors provide continuous monitoring of daily activities and movement patterns, offering insights into real-world function that complement clinic-based assessments. These devices can track steps, detect falls, monitor activity levels, and provide feedback about movement quality during daily activities. This information helps physiotherapists understand how well clinic gains translate to functional improvement.
The integration of artificial intelligence and machine learning in rehabilitation technology is enabling personalized treatment algorithms that adapt to individual patient responses. These systems can analyze movement patterns, predict optimal exercise progressions, and identify patients at risk for complications or poor outcomes.
Program Design and Progression Principles
Effective neurological physiotherapy programmes require systematic design principles that ensure appropriate challenge while maintaining safety and promoting optimal outcomes. The initial assessment forms the foundation for all subsequent programme development, requiring comprehensive evaluation of motor function, cognitive status, and individual goals.
Initial assessment protocols incorporate standardized outcome measures alongside clinical observation and patient-reported goals. The assessment typically includes evaluation of muscle strength using manual muscle testing or dynamometry, balance assessment using tools like the Berg Balance Scale, mobility evaluation through timed walking tests, and functional capacity assessment using activities of daily living scales. This comprehensive evaluation provides baseline data for programme development and outcome tracking.
Goal setting procedures involve collaborative discussions between patients, families, and the rehabilitation team to establish realistic, meaningful objectives. Goals should be specific, measurable, achievable, relevant, and time-bound (SMART), focusing on functional outcomes that matter to patients’ daily lives. For example, a goal might be “to walk independently for 50 meters within 8 weeks” rather than the more general “to improve walking.”
Exercise prescription parameters follow established principles adapted for neurological conditions. Frequency recommendations typically range from 3-5 sessions per week, with daily activities encouraged for balance and flexibility exercises. Intensity should be challenging but sustainable, generally targeting 60-70% of maximum capacity for cardiovascular exercises and progressing resistance training gradually. Duration begins with tolerance levels, often 20-30 minutes initially, progressing to 45-60 minutes as endurance improves.
Progressive overload principles require careful adaptation for neurological patients, as traditional strength training progressions may not be appropriate. Progression might involve increasing complexity rather than resistance, adding dual-task challenges, or advancing from supported to unsupported activities. The key is maintaining appropriate challenge while ensuring safety and movement quality.
Monitoring and adjustment strategies involve regular reassessment using the same outcome measures employed during initial evaluation. Progress should be documented weekly during intensive programmes, with formal reassessments monthly. Adjustments to exercise programmes should be based on objective improvements, patient feedback, and any changes in medical status or symptoms.
The transition from clinic-based to home-based exercise programmes requires careful planning and patient education. Patients must demonstrate competency in performing exercises safely and independently before transitioning to home programmes. Written instructions, exercise videos, and regular follow-up sessions support successful transition to independent exercise participation.

Home Exercise Programs and Self-Management
Home exercise programmes play a crucial role in maintaining and building upon gains achieved during formal rehabilitation. These programmes must balance effectiveness with safety, providing patients with structured activities they can perform independently while minimizing risk of injury or setbacks.
Essential exercises for home programmes typically focus on balance, flexibility, and functional movements that can be performed safely without specialized equipment. Balance exercises might include standing on one foot while holding onto a chair, walking heel-to-toe along a straight line, or standing from sitting without using hands for support. These activities can be progressed by reducing support or adding complexity as function improves.
Equipment recommendations for home-based neurological exercise emphasize safety and versatility. Basic equipment might include a sturdy chair for support, resistance bands for strength training, a therapy ball for balance challenges, and non-slip mats for floor exercises. More advanced equipment could include balance pads, light weights, or pedal exercisers, depending on individual needs and space constraints.
Caregiver training represents a critical component of successful home programmes, as family members often provide support and motivation for exercise participation. Caregivers learn to recognize proper exercise form, identify signs of fatigue or overexertion, and provide appropriate assistance when needed. Training should include hands-on practice with emergency procedures and clear guidelines about when to contact healthcare providers.
Self-monitoring techniques help patients track their progress and maintain motivation for continued exercise participation. Simple log books can record exercise completion, duration, and perceived difficulty. Patients might also monitor functional improvements, such as walking distance or balance confidence, to see the practical benefits of their exercise efforts. Technology solutions like smartphone apps can automate some monitoring functions while providing motivational feedback.
Progression guidelines for home programmes must be conservative to maintain safety while promoting continued improvement. Patients should be instructed to increase exercise duration before increasing intensity, and to progress only when current exercises can be completed easily and safely. Clear criteria for exercise advancement help patients make appropriate decisions about programme modifications.
Recognition of when to seek professional guidance ensures patient safety and optimal outcomes. Warning signs that require professional consultation include increased pain during or after exercise, new neurological symptoms, significant fatigue that doesn’t resolve with rest, or any falls or injuries during exercise. Regular check-ins with physiotherapists help monitor progress and make necessary programme adjustments.
The integration of home exercise programmes with daily activities enhances adherence and functional relevance. Patients might practice balance exercises while brushing teeth, perform calf raises while waiting for meals to cook, or practice coordination exercises during television viewing. This integration makes exercise feel less burdensome while promoting consistent participation.
Multidisciplinary Collaboration in Neurological Rehabilitation
Neurological rehabilitation requires coordinated efforts from multiple healthcare professionals, each contributing specialized expertise to address the complex needs of patients with neurological conditions. Physiotherapists play a central role within this team while collaborating closely with other disciplines to optimize patient outcomes.
The role of physiotherapists within the neurological rehabilitation team focuses primarily on movement, mobility, and physical function restoration. However, physiotherapists must also consider cognitive, communication, and psychosocial factors that influence movement and exercise participation. This holistic approach requires understanding of how other disciplines’ interventions complement and support physiotherapy goals.
Coordination with occupational therapists involves shared focus on functional activities, with physiotherapists addressing the movement components while occupational therapists focus on task adaptation and environmental modifications. For example, both disciplines might work on transfers, but physiotherapists emphasize the movement mechanics while occupational therapists address adaptive equipment and safety strategies.
Speech therapists contribute to neurological rehabilitation by addressing communication and swallowing difficulties that can impact exercise participation and safety. Physiotherapists must be aware of swallowing precautions that might affect hydration during exercise and communication strategies that facilitate effective interaction with patients who have speech impairments.
Integration with physicians ensures medical stability and optimal medication management to support exercise participation. Neurologists provide insights into disease progression and prognosis, while physiatrists coordinate rehabilitation goals and medical interventions. Physiotherapists must communicate exercise responses and any concerning symptoms to medical team members promptly.
Communication strategies for optimal patient outcomes include regular team meetings, shared documentation systems, and coordinated goal setting. Effective communication ensures that all team members understand each patient’s goals, limitations, and progress, preventing conflicting interventions and maximizing treatment efficiency. Electronic health records facilitate information sharing and coordination among team members.
Discharge planning requires collaborative efforts to ensure smooth transitions from inpatient to outpatient care or from formal rehabilitation to community-based services. The team must assess patients’ needs for continued therapy services, equipment requirements, and caregiver support. Community resource connections help patients access ongoing services like fitness programs, support groups, and adaptive sports opportunities.
The timing and sequencing of interventions from different disciplines can significantly impact outcomes. For example, patients might benefit from speech therapy sessions before physiotherapy to address communication needs, or occupational therapy might provide adaptive equipment that facilitates participation in physiotherapy exercises. Team coordination ensures optimal scheduling and intervention sequencing.
Quality improvement initiatives within multidisciplinary teams focus on measuring and improving patient outcomes through coordinated care approaches. Teams might track functional improvements, length of stay, and patient satisfaction to identify opportunities for enhanced collaboration and more effective interventions.
Frequently Asked Questions
Can neurological physiotherapy exercises be harmful if performed incorrectly?
Yes, incorrectly performed neurological exercises can potentially cause harm, which is why proper assessment and professional guidance are essential. Risks include falls due to inappropriate balance challenges, overexertion leading to fatigue or symptom worsening in conditions like multiple sclerosis, and development of abnormal movement patterns that can impede recovery. Specific risks for different conditions include autonomic dysreflexia in spinal cord injury patients and increased seizure risk in some brain injury patients. However, when properly prescribed and monitored by qualified neurological physiotherapists, exercise benefits far outweigh risks, with serious adverse events being rare.
How do I know if my neurological exercise program is working effectively?
Effective neurological exercise programs typically show measurable improvements within 4-6 weeks, though the timeline varies by condition and severity. Key indicators include improved performance on standardized tests like the Berg Balance Scale, increased walking speed or distance, reduced fall frequency, and enhanced ability to perform daily activities independently. Patients often report increased confidence in movement, better energy levels, and improved mood. Physiotherapists use objective outcome measures to track progress, including strength testing, balance assessments, and functional mobility tests. It’s important to note that progress may be gradual and sometimes plateaus occur, which doesn’t necessarily indicate programme failure but may require exercise modification.
What should I do if I experience increased fatigue or symptoms during exercises?
Increased fatigue or symptom worsening during exercise requires immediate attention and programme modification. Stop the exercise session immediately and rest until symptoms resolve. Contact your physiotherapist or healthcare provider if symptoms persist beyond normal recovery time or if you experience new symptoms like chest pain, severe shortness of breath, dizziness, or neurological changes. For patients with conditions like multiple sclerosis, temporary
Every person’s neurological journey is unique, which is why tailored exercise programmes and the right professional support make such a difference. If you’d like guidance on safe, structured rehabilitation for stroke recovery, multiple sclerosis, Parkinson’s disease, neurological physiotherapy page to see how we can help.
This article has been clinically reviewed for accuracy by Barry Ford, BSc (Hons), Chartered Physiotherapist.


